A 20-year-old man was found vomiting persistently at 3 a.m. He had emergency laparotomy 3 days before. The doctor on call earlier had prescribed anti-emetics for the patient, without carrying out a full assessment. The patient is extremely distressed now. The patient had undergone a ‘normal’ laparotomy for trauma. The small and large bowel were both examined carefully and no injury was found. He had made a good recovery and had been moved onto free fluids earlier in the day. There was no nasogastric tube left after the operation, and the urinary catheter had been removed.
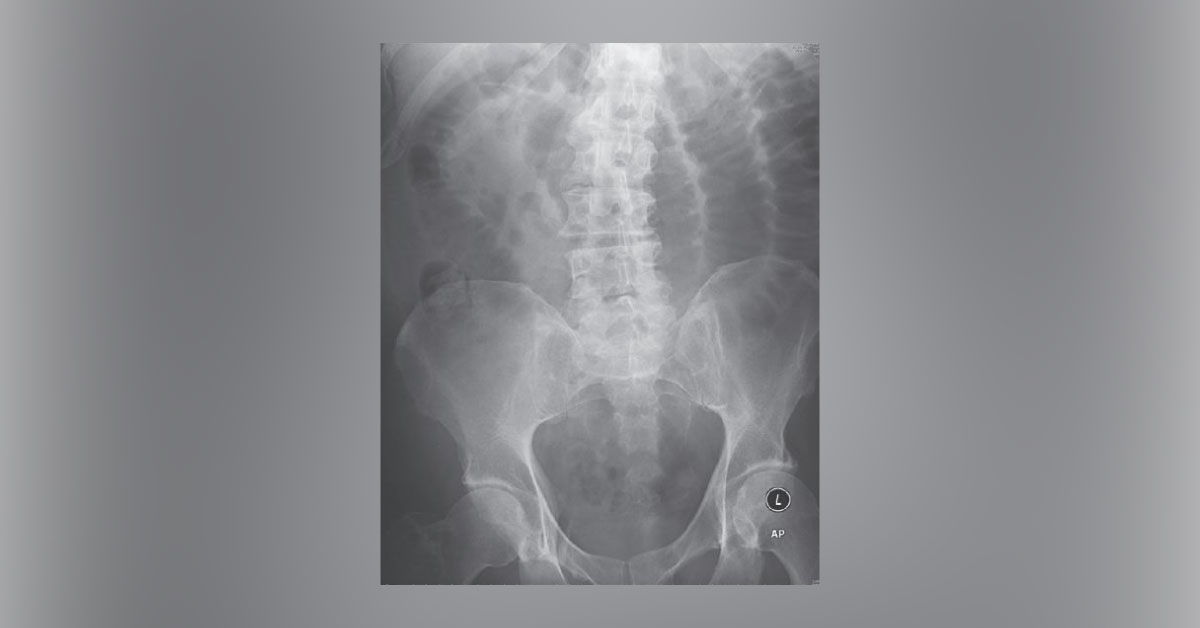
Examination The patient is rolling around in the bed having just vomited. His BP is 120/75 mmHg and pulse rate 110/min. He has a midline incision covered with a dry dressing. The abdomen is distended and tympanic. On palpation, he is tender around the incision only. There are no bowel sounds on auscultation. X-ray of…