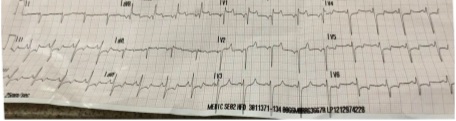
Case A 27-year-old male with a medical history of hypertension was taken to ED through emergency medical services. Upon arrival at the site, the emergency services defibrillated emergently resulting in immediate asystole. CPR was performed, and a return of spontaneous circulation (ROSC) was achieved. The rhythm strip showed significant ST segment elevations in V1-V2, AVL, and AVR; Q waves in V1–V2; diffuse ST depressions in II, III, AVF, and V3–V6 (as seen in the attached image).
On route to the hospital, the patient again developed acute asystole and CPR was initiated at arrival to the ER. Steps in ED Patient was pale, cold, severely cachectic, and volume depleted Central venous access was not possible whereas peripheral access was possible only for infusions but not for blood withdrawal Advanced cardiovascular life support (ACLS) was continued for approximately 40 min. but the…