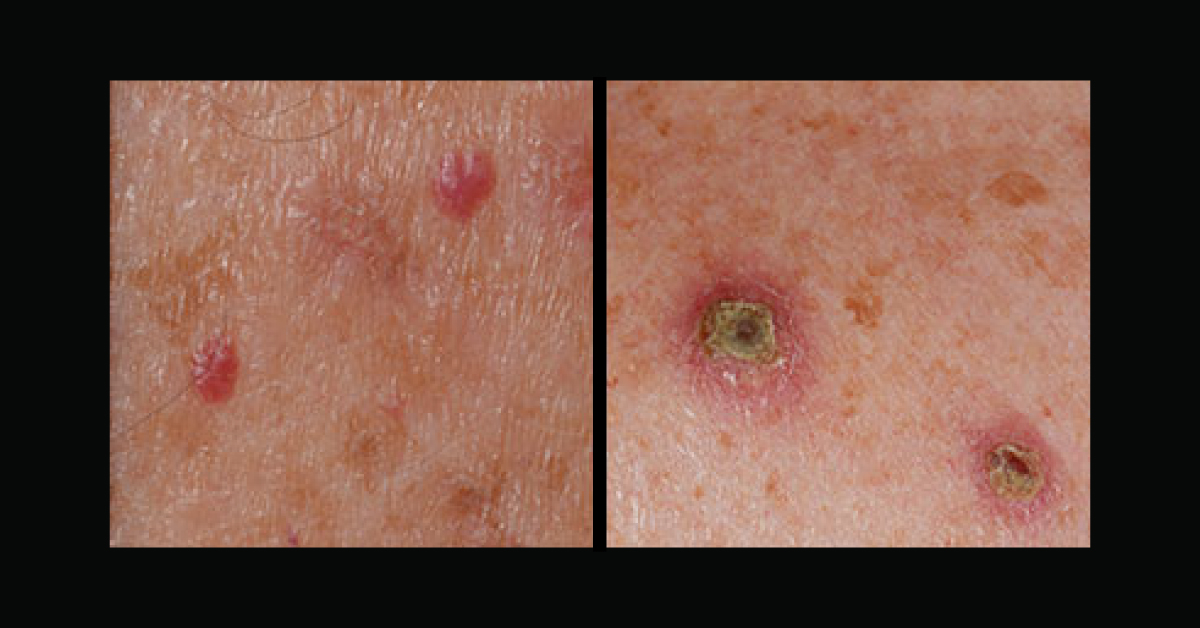
A 58-year-old man presented for review following a four-week trial of emollient, topical clobetasone butyrate 0.05% and oral antihistamine for a troublesome eczematous rash on his shins. The rash, which was initially patch-like, irregular and hyperkeratotic, had advanced to the chest and abdomen with dotted, itchy, red papules and friable pustules. In view of the non-responsive and atypical progression of the rash, the patient was referred to the rapid access dermatology clinic. The primary concern was a potential HIV-related skin condition or a paraneoplastic phenomenon.
Skin biopsy revealed features suspicious of necrolytic migratory erythema (NME). Blood tests showed Hb 109g/L, glycogen 348pmol/L (normal: 0-50pmol/L) and high chromagranin A and B (glycoprotein found in neuroendocrine tissue). He had an elevated oral glucose tolerance test and HbA1c of 52mmol/mol. During the next…