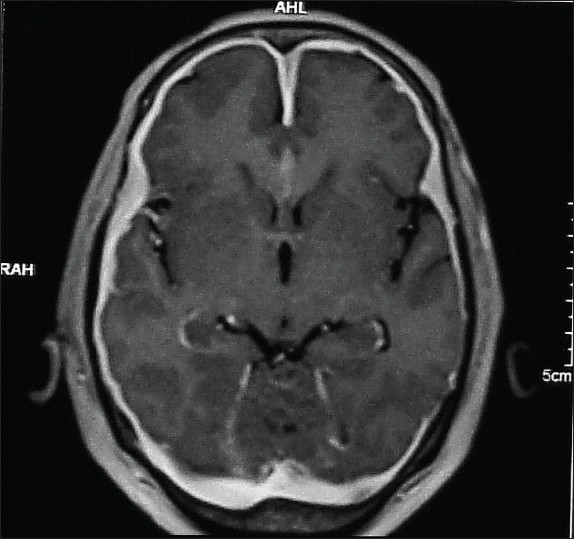
A 60-year-old woman with no history of any chronic illness presents with gradual loss of vision in both eyes since 6 months. She also has associated throbbing headache. Ophthalmic examination revealed absence of perception of light in both eyes. Fundoscopy reveals a hyperemic disc. She is non diabetic and normotensive with average build. She has mild arthralgia relieved by analgesics. Investigations reveal normal hematological and biochemistry parameters. X-ray chest was normal. Sputum AFB was negative. Rheumatoid Factor, anti-nuclear antibodies and anti dsDNA were negative. Serology was negative for HIV, VDRL and hepatitis B.
An MRI brain was taken. CSF analysis revealed mildly elevated proteins, normal cell counts and no evidence for tuberculosis. What is the abnormality? Source: Karthik, S. N et al. Annals of Indian Academy of Neurology 14.3 (2011): 203–204. PMC. Web. 2 Oct. 2016.