An 89-year-old female with stable chronic lymphocytic leukemia was presented to a hospital with dyspnea and dry cough. Except for sinus tachycardia, all vital signs were marked normal. Physical examination revealed anxiety, dyspnea, and sweat without fever. However, she was alert and well attentive. Investigation of the lung revealed reduced air entry with crackling sounds from the base of the lungs.
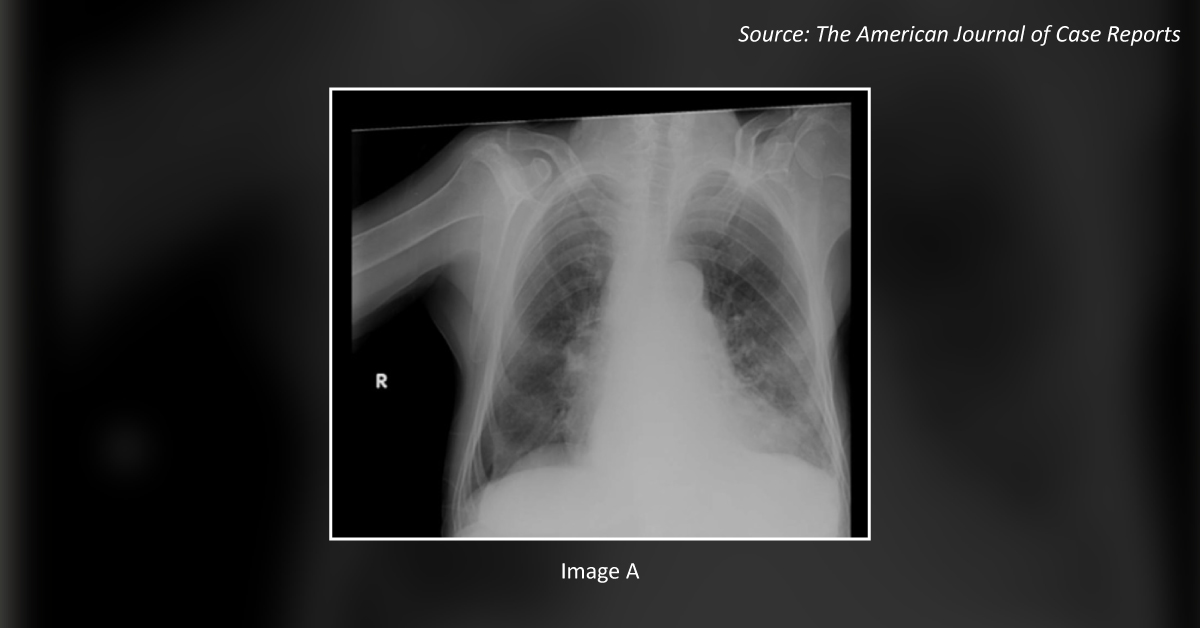
No peripheral edema and deep vein thrombosis were observed. The pulse rate was normal. Laboratory examination revealed leukocytosis; however, the hematological and biochemical parameters were unremarkable. Chest X-ray (CXR) showed enlarged cardiac silhouette, pulmonary congestion, and infiltration in the left lower lobe (Image A). Intravenous (IV) furosemide and antibiotics (IV ceftriaxone and oral azithromycin) were administered along with steroid therapy (methylprednisolone 62.5 mg, IV).…