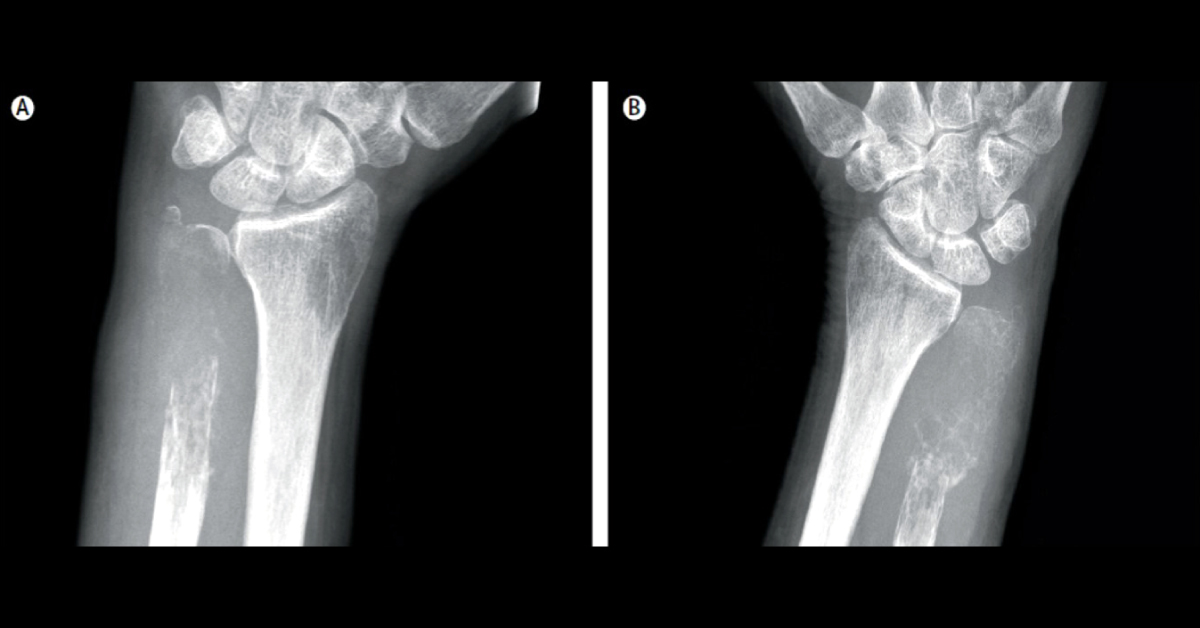
A 72-year-old man visited the surgical outpatient clinic with a spontaneous fracture of his left wrist. Exam Physical examination suggested an additional fracture of his right wrist. Conventional radiograph of both distal ulnae is attached as image. He reported no recent weight loss, night sweats, prostatic problems, or deteriorating performance status. There was no lymphadenopathy on physical examination.
Positron emission tomography : No primary tumour in the abdomen or thorax and no other skeletal lesions, nor was there any suspicion of prostate carcinoma. What should be next line of action? What is the cause of these isolated osteolytic lesions with no suspicion of prostate carcinoma? Source: The Lancet *This case is from Docplexus editorial team for educative purpose only