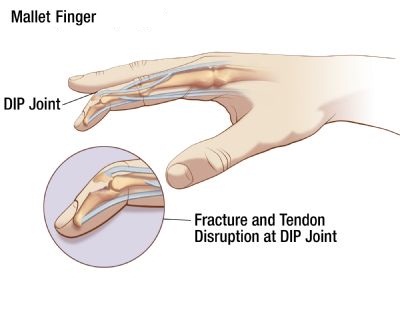
This is a flexion deformity affecting the distal interphalangeal joint of the finger and is due to either distal extensor tendon rupture or avulsion with a bony fragment after traumatic forced flexion of the extended fingertip. The resultant weakness is often painless and presents with an inability to actively extend the fingertip. Non-traumatic mallet finger occurs more often in diabetics.
Treatment is usually by splinting the distal interphalangeal joint in extension. Surgery is rarely required.