A 47-year-old woman with a history of hypertension presented to the emergency department after multiple episodes of palpitations with near syncope. While in the emergency department, she developed monomorphic ventricular tachycardia (VT) with hemodynamic instability and was successfully cardioverted. She continued to have non-sustained monomorphic VT, so intravenous amiodarone and oral metoprolol were initiated. She was admitted for further evaluation.
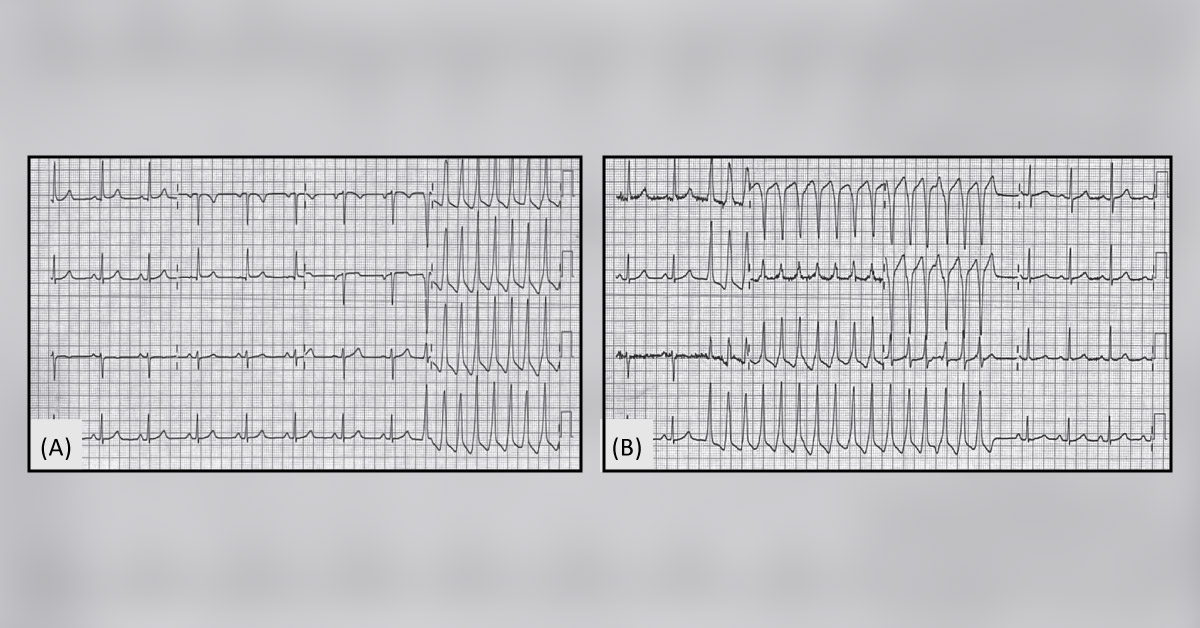
The electrolyte levels and coronary angiography were found to be normal. Cardiac MRI with gadolinium contrast revealed normal-sized cardiac chambers and normal biventricular function without delayed enhancement. The presenting electrocardiogram and patient electrocardiogram on the development of a wide complex monomorphic tachycardia rhythm (ECG) were studied (Image A and B, respectively). Source : JAMA Cardiology Clinical Challenge…