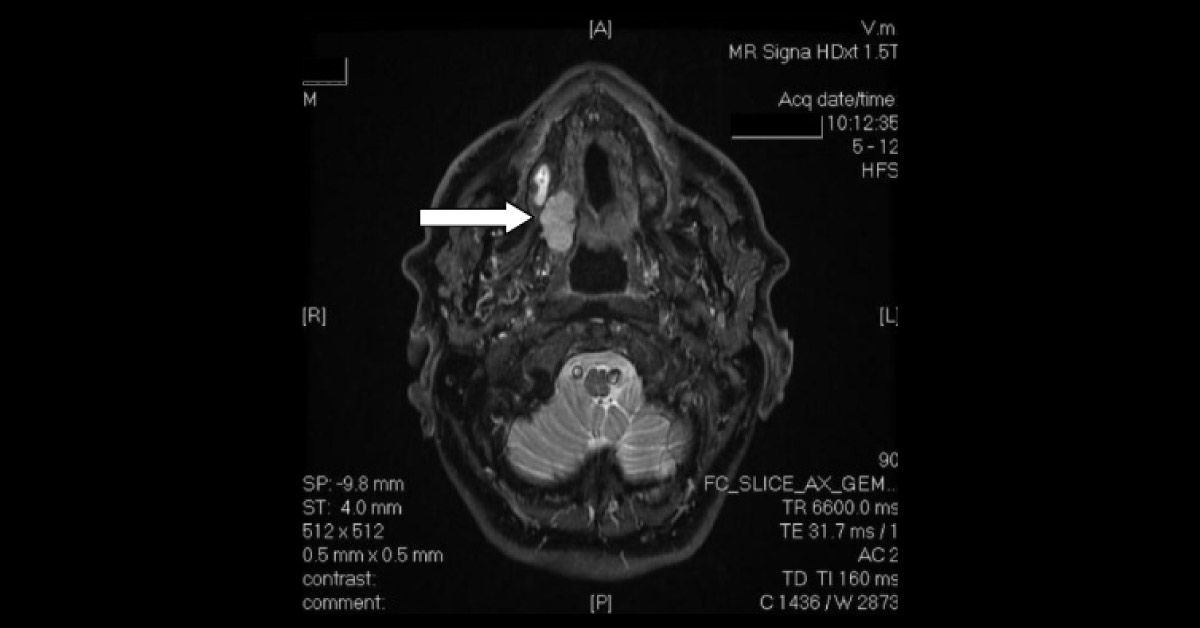
A 74-year-old male with a history of smoking presented with adenocarcinoma of the right palatomaxillary region (image) and was scheduled for maxillectomy. He also had a history of COPD, mild aortic insufficiency, and incomplete right bundle-branch block on ECG. Anesthesia was uneventful - premedication with oxazepam, induction with propofol, sufentanil, rocuronium, and maintenance with sevoflurane and N 2 O. The airway was secured by endotracheal intubation through the nasal route.
To scavenge intraoperative blood and tissue debris, which could enter the larynx or esophagus, the pharynx was packed with gauze using the Magill-type forceps. At the end of the surgery, the gauge was removed and the surgical site was rechecked for adequate hemostasis. The sevoflurane and N 2 O were then stopped. The patient was allowed to awaken and was extubated only after the return of protective airway…